
Chronic myeloid leukemia
Updates to Article Attributes
Chronic myeloid leukemia, also known as chronic myelogenous leukemia, is a myeloproliferative neoplasm characterized by the overproduction of differentiated granulocytesgranulocytes with fairly normal differentiation.
Epidemiology
The annual incidence is about 1 per 100,000 1. The typical age at presentation is 50-60 years 1.
Clinical presentation
Constitutional symptoms are common, such as fatigue, weight loss, and sweats 2. Some patients are asymptomatic, with the diagnosis being first suspected based upon routine blood work finding leukocytosis with a predominance of the neutrophil lineage.
Pathology
Genetics
Chronic myeloid leukemia is caused by a chromosomal abnormality in hematopoietic stem cells in which reciprocal translocation between chromosomes 9 and 22 creates the fusion gene BCR-ABL1. The shortened chromosome 22 containing the fusion gene is called the Philadelphia chromosome. The diagnosis is established by karyotype (to detect the Philadelphia chromosome), fluorescence in situ hybridization (to detect the BCR-ABL1 fusion gene), or reverse transcription polymerase chain reaction (to detect the BCR-ABL1 mRNA product).
Radiographic features
Patients commonly have splenomegaly and diffuse marrow infiltration (manifest as abnormally low signal on T1-weighted MRI).
Treatment and prognosis
First-line medical therapy consists of tyrosine kinase inhibitors (imatinib, dasatinib, or nilotinib) 1. With tyrosine kinase inhibitor treatment, life expectancy approaches that of the general population. In some treated patients and in untreated patients, the disease progresses over several years through an accelerated phase and culminates in a blast phase (or blast crisis), which represents a fatal acute leukemia.
See also
-<p><strong>Chronic myeloid leukemia</strong>, also known as <strong>chronic myelogenous </strong><strong>leukemia</strong>, is a <a title="Myeloproliferative neoplasm" href="/articles/myeloproliferative-neoplasm-1">myeloproliferative neoplasm</a> characterized by the overproduction of differentiated granulocytes.</p><h4>Epidemiology</h4><p>The annual incidence is about 1 per 100,000 <sup>1</sup>. The typical age at presentation is 50-60 years <sup>1</sup>.</p><h4>Clinical presentation</h4><p>Constitutional symptoms are common, such as fatigue, weight loss, and sweats <sup>2</sup>. Some patients are asymptomatic, with the diagnosis being first suspected based upon routine blood work finding leukocytosis with a predominance of the neutrophil lineage.</p><h4>Pathology</h4><h5>Genetics</h5><p>Chronic myeloid leukemia is caused by a chromosomal abnormality in hematopoietic stem cells in which reciprocal translocation between chromosomes 9 and 22 creates the fusion gene <em>BCR-ABL1</em>. The shortened chromosome 22 containing the fusion gene is called the Philadelphia chromosome. The diagnosis is established by karyotype (to detect the Philadelphia chromosome), fluorescence in situ hybridization (to detect the <em>BCR-ABL1</em> fusion gene), or reverse transcription polymerase chain reaction (to detect the <em>BCR-ABL1 </em>mRNA product).</p><h4>Radiographic features</h4><p>Patients commonly have <a title="Splenomegaly" href="/articles/splenomegaly">splenomegaly</a> and diffuse marrow infiltration (manifest as abnormally low signal on T1-weighted MRI).</p><h4>See also</h4><ul><li><a title="WHO classification of tumours of haematopoietic and lymphoid tissues" href="/articles/who-classification-of-tumours-of-haematopoietic-and-lymphoid-tissues-1">WHO classification of tumours of haematopoietic and lymphoid tissues</a></li></ul>- +<p><strong>Chronic myeloid leukemia</strong>, also known as <strong>chronic myelogenous </strong><strong>leukemia</strong>, is a <a href="/articles/myeloproliferative-neoplasm-1">myeloproliferative neoplasm</a> characterized by the overproduction of granulocytes with fairly normal differentiation.</p><h4>Epidemiology</h4><p>The annual incidence is about 1 per 100,000 <sup>1</sup>. The typical age at presentation is 50-60 years <sup>1</sup>.</p><h4>Clinical presentation</h4><p>Constitutional symptoms are common, such as fatigue, weight loss, and sweats <sup>2</sup>. Some patients are asymptomatic, with the diagnosis being first suspected based upon routine blood work finding leukocytosis with a predominance of the neutrophil lineage.</p><h4>Pathology</h4><h5>Genetics</h5><p>Chronic myeloid leukemia is caused by a chromosomal abnormality in hematopoietic stem cells in which reciprocal translocation between chromosomes 9 and 22 creates the fusion gene <em>BCR-ABL1</em>. The shortened chromosome 22 containing the fusion gene is called the Philadelphia chromosome. The diagnosis is established by karyotype (to detect the Philadelphia chromosome), fluorescence in situ hybridization (to detect the <em>BCR-ABL1</em> fusion gene), or reverse transcription polymerase chain reaction (to detect the <em>BCR-ABL1 </em>mRNA product).</p><h4>Radiographic features</h4><p>Patients commonly have <a href="/articles/splenomegaly">splenomegaly</a> and diffuse marrow infiltration (manifest as abnormally low signal on T1-weighted MRI).</p><h4>Treatment and prognosis</h4><p>First-line medical therapy consists of tyrosine kinase inhibitors (imatinib, dasatinib, or nilotinib) <sup>1</sup>. With tyrosine kinase inhibitor treatment, life expectancy approaches that of the general population. In some treated patients and in untreated patients, the disease progresses over several years through an accelerated phase and culminates in a blast phase (or blast crisis), which represents a fatal acute leukemia.</p><h4>See also</h4><ul><li><a href="/articles/who-classification-of-tumours-of-haematopoietic-and-lymphoid-tissues-1">WHO classification of tumours of haematopoietic and lymphoid tissues</a></li></ul>
References changed:
- 1. Hochhaus A, Saussele S, Rosti G, Mahon FX, Janssen JJWM, Hjorth-Hansen H, Richter J, Buske C. Chronic myeloid leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. (2017) Annals of oncology : official journal of the European Society for Medical Oncology. 28 (suppl_4): iv41-iv51. <a href="https://doi.org/10.1093/annonc/mdx219">doi:10.1093/annonc/mdx219</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/28881915">Pubmed</a> <span class="ref_v4"></span>
- 2. Savage DG, Szydlo RM, Goldman JM. Clinical features at diagnosis in 430 patients with chronic myeloid leukaemia seen at a referral centre over a 16-year period. (1997) British journal of haematology. 96 (1): 111-6. <a href="https://www.ncbi.nlm.nih.gov/pubmed/9012696">Pubmed</a> <span class="ref_v4"></span>
Systems changed:
- Haematology
Image 1 MRI (Coronal) ( create )
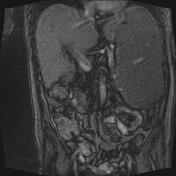
Image 2 MRI (T1) ( create )

Image 3 MRI (T1) ( create )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.