
Hydrocephalus
Updates to Article Attributes
Hydrocephalus merely denotes an increase in the volume of CSF and thus of the cerebral ventricles.
Although hydrocephalus is often divided into obstructive and communicating typestypically referred to as either being "obstructive" or "communicating", this can lead to confusion as to the underlying cause of ventriculomegaly, as the terms are referring to different aspects of the underlying pathophysiology (names why and where). For example, acute subarachnoid haemorrhage confined to the basal cisterns can result in ventriculomegaly by obstructing the normal flow of CSF through the basal cisterns, and by filling the arachnoid granulations. Given that this is mechanistically an obstruction to CSF flow outside of the ventricular system should it be considered communicating or obstructive hydrocephalus? The correct answer is that in that example it would be communicating obstructive hydrocephalus.
As such a more precise terminology is to divide hydrocephalus into:
- communicating and non-communicating: addressing where the obstruction is located
- obstructive and non-obstructive
(on: on the grounds of whether or not there isobstuctionobstruction of CSF pathways in the ventricles or in the subarachnoid space) as well as into communicating and non-communicating (addressing where the obstruction is located)1-3.
This nomenclature leads to the following types of hydrocephalus (see figures 1 & 2):
-
obstructive hydrocephalus(passage ofwithincan exit the ventricular systemor in the subarachnoid space is impaired at some point)-
communicating obstructive hydrocephaluswith obstruction to CSF absorption-
often merelyusually referred to merely as communicating hydrocephalus - passage of CSF from the ventricular system
andinto the subarachnoid space is unimpeded butabsorption of CFS viaat some point between the basal cisterns and the arachnoid granulations, normal flow isimpairedimpeded.- subarachnoid haemorrhage (obstruction can be acute to to filling of the basal cisterns with blood clot, or chronic due to scarring of the subarachnoid space and arachnoid granulations)
-
most commonly seen as a result ofsubarachnoid haemorrhageor- TB meningitis is typically basal filling the basal cisterns
- bacterial meningitis is typically also over the convexities
-
extra-axialleptomeningeal carcinomatosis
-
-
without obstruction to CSF
spaces (e.g. Sylvian fissuresabsorption-
a special group of conditions with disparate, and
sulci) are also distended
often poorly understood, abnormal CSF dynamics, including: - normal pressure hydrocephalus (NPH)
- choroid plexus papillomas (
-
part of the associated hydrocephalus is
a specific subtypethought to be due to over production ofcommunicatingCSF 1. An obstructive component in larger masses is often also present)
-
a special group of conditions with disparate, and
-
additionally, other conditions with large ventricles fall into this group although they are often not thought of as hydrocephalus
, which remains poorly understood.. These include:- hydrocephalus ex-vacuo and colpocephaly (ventricles are enlarged due to loss of adjacent brain parenchyma)
-
- often merely referred to asobstructive hydrocephalus
-
due to obstruction of CSF out flow at any point (e.g.aqueduct stenosis,colloid cystobstructing theforamen of Monro) - up-stream ventricles are dilated and exert mass effect upon adjacent brain (e.g. effacement of sulci)
-
numerous causes including:
- foramen of Monro: colloid cyst
- aqueduct of Sylvius: aqueduct stenosis, tectal glioma
- fourth ventricle: posterior fossa tumour, or cerebellar infarct or cerebellar haemorrhage
-
often referred to asex-vacuo dilatation of the ventricles CSF can pass out of the ventricles and into the basal cisterns without impediment, and is readily absorbedventricles are enlarged due to loss of adjacent brain parenchyma
It should be noted that in the above examples CSF production is either normal or reduced as a result of decreased absorption of CSF. Increase in production of CSF rarely plays a role, with the partial exception is choroid plexus papillomas in which part of the associated hydrocephalus is thought to be due to over production of CSF 1.
-<p><strong>Hydrocephalus</strong> merely denotes an increase in the volume of CSF and thus of the <a href="/articles/ventricular-system">cerebral ventricles</a>. </p><p>Although hydrocephalus is often divided into obstructive and communicating types, this can lead to confusion as the terms are referring to different aspects of the underlying pathophysiology (names why and where). As such a more precise terminology is to divide hydrocephalus into obstructive and non-obstructive (on the grounds of whether or not there is obstuction of CSF pathways in the ventricles or in the subarachnoid space) as well as into communicating and non-communicating (addressing where the obstruction is located) <sup>1-3.</sup> This nomenclature leads to the following types of hydrocephalus:</p><ul>- +<p><strong>Hydrocephalus</strong> merely denotes an increase in the volume of CSF and thus of the <a href="/articles/ventricular-system">cerebral ventricles</a>. </p><p>Although hydrocephalus is typically referred to as either being "obstructive" or "communicating", this can lead to confusion as to the underlying cause of ventriculomegaly, as the terms are referring to different aspects of the underlying pathophysiology (names why and where). For example, acute subarachnoid haemorrhage confined to the basal cisterns can result in ventriculomegaly by obstructing the normal flow of CSF through the basal cisterns, and by filling the arachnoid granulations. Given that this is mechanistically an obstruction to CSF flow outside of the ventricular system should it be considered communicating or obstructive hydrocephalus? The correct answer is that in that example it would be communicating obstructive hydrocephalus. </p><p>As such a more precise terminology is to divide hydrocephalus into:</p><ol>
- +<li>communicating and non-communicating: addressing where the obstruction is located</li>
- +<li>obstructive and non-obstructive: on the grounds of whether or not there is obstruction of CSF pathways in the ventricles or in the subarachnoid space <sup>1-3.</sup>
- +</li>
- +</ol><p>This nomenclature leads to the following types of hydrocephalus (see figures 1 & 2):</p><ul>
- +<li>communicating (ie CSF can exit the ventricular system)<ul>
- +<li>with obstruction to CSF absorption<ul>
- +<li>usually referred to merely as <a title="Communicating hydrocephalus" href="/articles/obstructive-hydrocephalus">communicating hydrocephalus</a>
- +</li>
- +<li>passage of CSF from the ventricular system into the subarachnoid space is unimpeded but at some point between the basal cisterns and the arachnoid granulations, normal flow is impeded. <ul>
- +<li>
- +<a href="/articles/subarachnoid-haemorrhage">subarachnoid haemorrhage</a> (obstruction can be acute to to filling of the basal cisterns with blood clot, or chronic due to scarring of the subarachnoid space and arachnoid granulations)</li>
- +<li>infective <a href="/articles/meningitis">meningitis</a> (both during infection and chronic) <ul>
-<a href="/articles/obstructive-hydrocephalus">obstructive hydrocephalus</a> (passage of CSF within the ventricular system or in the subarachnoid space is impaired at some point)<ul>-<li>communicating obstructive hydrocephalus<ul>-<li>often merely referred to as <strong>communicating hydrocephalus</strong>- +<a href="/articles/tuberculous-meningitis">TB meningitis</a> is typically basal filling the basal cisterns</li>
- +<li>bacterial meningitis is typically also over the convexities</li>
- +</ul>
-<li>passage of CSF from the ventricular system and into the subarachnoid space is unimpeded but absorption of CFS via arachnoid granulations is impaired</li>-<li>most commonly seen as a result of <a href="/articles/subarachnoid-haemorrhage">subarachnoid haemorrhage</a> or <a href="/articles/meningitis">meningitis</a>- +<li><a href="/articles/leptomeningeal-metastases">leptomeningeal carcinomatosis</a></li>
- +</ul>
-<li>extra-axial CSF spaces (e.g. Sylvian fissures and sulci) are also distended</li>- +</ul>
- +</li>
- +<li>without obstruction to CSF absorption<ul>
- +<li>a special group of conditions with disparate, and often poorly understood, abnormal CSF dynamics, including:<ul>
- +<li><a href="/articles/normal-pressure-hydrocephalus">normal pressure hydrocephalus (NPH)</a></li>
-<a href="/articles/normal-pressure-hydrocephalus">normal pressure hydrocephalus (NPH)</a> is a specific subtype of communicating hydrocephalus, which remains poorly understood. </li>- +<a href="/articles/choroid-plexus-papilloma-1">choroid plexus papillomas</a> (</li>
- +<li>part of the associated hydrocephalus is thought to be due to over production of CSF <sup>1</sup>. An obstructive component in larger masses is often also present)</li>
-<li>non-communicating obstructive hydrocephalus<ul>-<li>often merely referred to as <strong>obstructive hydrocephalus</strong>- +<li>additionally, other conditions with large ventricles fall into this group although they are often not thought of as hydrocephalus. These include:<ul><li>
- +<a href="/articles/hydrocephalus-ex-vacuo">hydrocephalus ex-vacuo</a> and <a href="/articles/colpocephaly">colpocephaly</a> (ventricles are enlarged due to loss of adjacent brain parenchyma)</li></ul>
-<li>due to obstruction of CSF out flow at any point (e.g. <a href="/articles/aqueduct-stenosis">aqueduct stenosis</a>, <a href="/articles/colloid-cyst-of-the-third-ventricle">colloid cyst</a> obstructing the <a title="Foramen of Monro" href="/articles/interventricular-foramen-of-monro">foramen of Monro</a>)</li>-<li>up-stream ventricles are dilated and exert mass effect upon adjacent brain (e.g. effacement of sulci)</li>-<li>non-obstructive hydrocephalus<ul>-<li>often referred to as <strong>ex-vacuo dilatation of the ventricles</strong>- +<li>non-communicating (ie CSF cannot exit the ventricular system - and thus there is by definition obstruction to CSF absorption)<ul>
- +<li>often merely referred to as <a href="/articles/obstructive-hydrocephalus">obstructive hydrocephalus</a>
- +</li>
- +<li>up-stream ventricles are dilated and exert mass effect upon adjacent brain (e.g. effacement of sulci)</li>
- +<li>numerous causes including:<ul>
- +<li>
- +<a href="/articles/foramen-of-monro">foramen of Monro</a>: <a href="/articles/colloid-cyst-of-the-third-ventricle">colloid cyst</a>
- +</li>
- +<li>
- +<a href="/articles/cerebral-aqueduct-of-sylvius">aqueduct of Sylvius</a>: <a href="/articles/aqueduct-stenosis">aqueduct stenosis</a>, <a href="/articles/tectal-glioma">tectal glioma</a> </li>
- +<li>fourth ventricle: <a href="/articles/posterior-fossa-tumours">posterior fossa tumour</a>, or <a href="/articles/cerebellar-infarction">cerebellar infarct</a> or <a href="/articles/cerebellar-haemorrhage">cerebellar haemorrhage</a>
- +</li>
- +</ul>
-<li>CSF can pass out of the ventricles and into the basal cisterns without impediment, and is readily absorbed</li>-<li>ventricles are enlarged due to loss of adjacent brain parenchyma</li>-</ul><p>It should be noted that in the above examples CSF production is either normal or reduced as a result of decreased absorption of CSF. Increase in production of CSF rarely plays a role, with the partial exception is <a href="/articles/choroid-plexus-papilloma-1">choroid plexus papillomas</a> in which part of the associated hydrocephalus is thought to be due to over production of CSF <sup>1</sup>. </p>- +</ul>
Image 1 ( create )
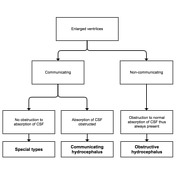
Image 2 ( create )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.