Intracranial teratoma
Updates to Article Attributes
Intracranial teratomas are uncommon intracranial neoplasms, which can have a bewildering variety of components and thus a wide range of appearances. TheyThey can be divided into two broad categories, intraintra and extra-axial, which differ in epidemiology and clinical presentation. Another method of classifying an intracranial teratoma is as mature, immature and mature with with malignant transformation.
Epidemiology
Although uncommon in the general population, they account for the largest proportion of fetal intracranial neoplasms ( 26 - 50(26-50% of fetal brain tumours 3,6)
Clinical presentation
Clinical presentation varies according to whether they are intra- or extra-axial.
Intra-axial
Intra-axial teratomas, i.e. those located within the cerebral hemispheres, typically present either antenatally or in the newborn period. They are large tumours that increase head circumference and therefore often present with difficulty in child birth. They tend to more commonly occur supratentorially.
Extra-axial
Extra axial teratomas usually present in childhood or early adulthood and are typically smaller. They most commonly arise in the pineal or suprasellar regions, and present due to mass effect: obstructive hydrocephalus due to impingement on the mid brain, Parinaud's syndrome, optic chiasm compression etc...
Pathology
Teratomas are considered intracranial germ cell tumours, and are comprised of cells originating from at least two and usually all three embryonic layers: ectoderm, mesoderm and endoderm. The histological sub type may not necessarily determine the biological behaviour.
Sometimes may be associated with elevated levels of:
Radiographic features
Intracranial teratomas are often seen as large lesions at presentation.
Given their extremely variable histological components, imaging also tends to be heterogenous, with tumours typically demonstrating a mixture of tissue densities and signal intensity. Fat, if present is helpful in narrowing the differential.
CT
The majority of intracranial teratomas demonstrate at least some fat and some calcification, which is usually solid/"clump like" 4,6. They usually have cystic and solid components, contributing to an irregular outline. Solid components demonstrate variable enhancement 4.
MRI
-
T1
- hyperintense components due to fat and proteinaceous
/ lipid/lipid rich fluid - intermediate components of soft tissue
- hypointense components due to calcification and blood products
- hyperintense components due to fat and proteinaceous
-
T1 C+ (Gd):
) :solid soft tissue components show enhancement -
T2:
:again mixed signal from differing components
Treatment and prognosis
Location and size determines prognosis.
In intra-axial (fetal) cases, stillbirth occurs relatively frequently, and difficulty with vaginal delivery (if attempted) can occur due to enlarged cranial circumference 3.
In extra-axial cases it largely depends on the size and location. Smaller lesions can be successfully resected with good prognosis.
Differential diagnosis
A meaningful differential depends to a degree on location.
- intra-axial
- sPNET
- atypical rhabdoid / teratoid tumour (ATRT): older age group
- choroid plexus carcinoma
- extra-axial
- intracranial lipoma: fatty components only
- intracranial dermoid: more mature tissue
- craniopharyngioma: particularly for suprasellar lesions
- other pineal region tumours
-<p><strong>Intracranial teratomas</strong> are uncommon intracranial neoplasms, which can have a bewildering variety of components and thus a wide range of appearances. They can be divided into two broad categories, intra and extra-axial, which differ in epidemiology and clinical presentation. Another method of classifying an intracranial teratoma is as mature, immature and mature with with malignant transformation.</p><h4>Epidemiology</h4><p>Although uncommon in the general population, they account for the largest proportion of <a title="Fetal brain tumors" href="/articles/fetal-brain-tumours">fetal intracranial neoplasms</a> ( 26 - 50% of fetal brain tumours <sup>3,6</sup>)</p><h4>Clinical presentation</h4><p>Clinical presentation varies according to whether they are intra- or extra-axial. </p><h5>Intra-axial </h5><p>Intra-axial teratomas, i.e. those located within the cerebral hemispheres, typically present either antenatally or in the newborn period. They are large tumours that increase head circumference and therefore often present with difficulty in child birth. They tend to more commonly occur supratentorially.</p><h5>Extra-axial </h5><p>Extra axial teratomas usually present in childhood or early adulthood and are typically smaller. They most commonly arise in the pineal or suprasellar regions, and present due to mass effect: <a title="Obstructive hydrocephalus" href="/articles/obstructive_hydrocephalus">obstructive hydrocephalus</a> due to impingement on the mid brain, <a title="Parinaud Syndrome" href="/articles/parinaud-syndrome">Parinaud's syndrome</a>, optic chiasm compression etc...</p><h4>Pathology</h4><p>Teratomas are considered <a href="/articles/intracranial-germ-cell-tumours">intracranial germ cell tumours</a>, and are comprised of cells originating from at least two and usually all three embryonic layers : ectoderm, mesoderm and endoderm. The histological sub type may not necessarily determine the biological behaviour. </p><p>Sometimes may be associated with elevated levels of:</p><ul>-<li>serum <a title="Conditions associated with raised alpha feto protein" href="/articles/altered-alpha-fetoprotein-levels">alpha feto protein (AFP)</a> </li>-<li>serum <a title="carcinoembryonic antigen (CEA)" href="/articles/carcinoembryonic-antigen-cea">carcinoembryonic antigen (CEA)</a> </li>-</ul><h4>Radiographic features</h4><p>Intracranial teratomas are often seen as large lesions at presentation. </p><p>Given their extremely variable histological components, imaging also tends to be heterogenous, with tumours typically demonstrating a mixture of tissue densities and signal intensity. Fat, if present is helpful in narrowing the differential. </p><h5>CT</h5><p>The majority of intracranial teratomas demonstrate at least some fat and some calcification, which is usually solid / "clump like" <sup>4,6</sup>. They usually have cystic and solid components, contributing to an irregular outline. Solid components demonstrate variable enhancement <sup>4</sup>. </p><h5>MRI</h5><ul>-<li>- +<p><strong>Intracranial teratomas</strong> are uncommon intracranial neoplasms, which can have a bewildering variety of components and thus a wide range of appearances. They can be divided into two broad categories, intra and extra-axial, which differ in epidemiology and clinical presentation. Another method of classifying an intracranial teratoma is as mature, immature and mature with with malignant transformation.</p><h4>Epidemiology</h4><p>Although uncommon in the general population, they account for the largest proportion of <a href="/articles/fetal-brain-tumours">fetal intracranial neoplasms</a> (26-50% of fetal brain tumours <sup>3,6</sup>)</p><h4>Clinical presentation</h4><p>Clinical presentation varies according to whether they are intra- or extra-axial. </p><h5>Intra-axial </h5><p>Intra-axial teratomas, i.e. those located within the cerebral hemispheres, typically present either antenatally or in the newborn period. They are large tumours that increase head circumference and therefore often present with difficulty in child birth. They tend to more commonly occur supratentorially.</p><h5>Extra-axial </h5><p>Extra axial teratomas usually present in childhood or early adulthood and are typically smaller. They most commonly arise in the pineal or suprasellar regions, and present due to mass effect: <a href="/articles/obstructive-hydrocephalus">obstructive hydrocephalus</a> due to impingement on the mid brain, <a href="/articles/parinaud-syndrome">Parinaud's syndrome</a>, optic chiasm compression etc...</p><h4>Pathology</h4><p>Teratomas are considered <a href="/articles/intracranial-germ-cell-tumours">intracranial germ cell tumours</a>, and are comprised of cells originating from at least two and usually all three embryonic layers: ectoderm, mesoderm and endoderm. The histological sub type may not necessarily determine the biological behaviour. </p><p>Sometimes may be associated with elevated levels of:</p><ul>
- +<li>serum <a href="/articles/afp-elevation">alpha feto protein (AFP)</a>
- +</li>
- +<li>serum <a href="/articles/carcinoembryonic-antigen-cea">carcinoembryonic antigen (CEA)</a>
- +</li>
- +</ul><h4>Radiographic features</h4><p>Intracranial teratomas are often seen as large lesions at presentation. </p><p>Given their extremely variable histological components, imaging also tends to be heterogenous, with tumours typically demonstrating a mixture of tissue densities and signal intensity. Fat, if present is helpful in narrowing the differential.</p><h5>CT</h5><p>The majority of intracranial teratomas demonstrate at least some fat and some calcification, which is usually solid/"clump like" <sup>4,6</sup>. They usually have cystic and solid components, contributing to an irregular outline. Solid components demonstrate variable enhancement <sup>4</sup>. </p><h5>MRI</h5><ul>
- +<li>
-<li>hyperintense components due to fat and proteinaceous / lipid rich fluid</li>-<li>intermediate components of soft tissue</li>-<li>hypointense components due to calcification and blood products</li>- +<li>hyperintense components due to fat and proteinaceous/lipid rich fluid</li>
- +<li>intermediate components of soft tissue</li>
- +<li>hypointense components due to calcification and blood products</li>
-</li>-<li>-<strong>T1 C+ (Gd</strong>) : solid soft tissue components show enhancement</li>-<li>-<strong>T2</strong> : again mixed signal from differing components</li>- +</li>
- +<li>
- +<strong>T1 C+ (Gd):</strong> solid soft tissue components show enhancement</li>
- +<li>
- +<strong>T2:</strong> again mixed signal from differing components</li>
-<li>intra-axial-<ul>-<li><a title="supratentorial primitive neuroectodermal tumour (sPNET)" href="/articles/primitive-neuroectodermal-tumour-of-the-cns">sPNET</a></li>-<li>-<a title="Atypical teratoid / rhabdoid tumour (AT/RT)" href="/articles/atypical-teratoid-rhabdoid-tumour">atypical rhabdoid / teratoid tumour (ATRT) </a>: older age group</li>-<li><a title="Choroid plexus carcinoma (CPC)" href="/articles/choroid-plexus-carcinoma">choroid plexus carcinoma</a></li>- +<li>intra-axial<ul>
- +<li><a href="/articles/primitive-neuroectodermal-tumour-of-the-cns">sPNET</a></li>
- +<li>
- +<a href="/articles/atypical-teratoidrhabdoid-tumour">atypical rhabdoid / teratoid tumour (ATRT)</a>: older age group</li>
- +<li><a href="/articles/choroid-plexus-carcinoma">choroid plexus carcinoma</a></li>
-</li>-<li>extra-axial-<ul>-<li>-<a title="Intracranial lipoma" href="/articles/intracranial_lipoma">intracranial lipoma</a> : fatty components only</li>-<li>-<a title="Dermoid cyst (CNS + Head and Neck)" href="/articles/intracranial-dermoid-cyst-1">intracranial dermoid</a> : more mature tissue</li>-<li>-<a title="Craniopharyngioma" href="/articles/craniopharyngioma">craniopharyngioma</a> : particularly for suprasellar lesions</li>-<li>other <a title="Pineal masses" href="/articles/pineal-region-mass">pineal region tumours</a> </li>- +</li>
- +<li>extra-axial<ul>
- +<li>
- +<a href="/articles/intracranial-lipoma">intracranial lipoma</a>: fatty components only</li>
- +<li>
- +<a href="/articles/intracranial-dermoid-cyst-1">intracranial dermoid</a>: more mature tissue</li>
- +<li>
- +<a href="/articles/craniopharyngioma">craniopharyngioma</a>: particularly for suprasellar lesions</li>
- +<li>other <a href="/articles/pineal-region-mass">pineal region tumours</a>
- +</li>
-</li>- +</li>
Image 1 MRI (T1 C+) ( update )
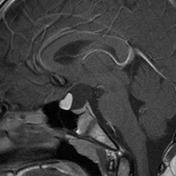
Image 2 MRI (T1) ( update )

Image 3 MRI (T1) ( update )

Image 4 MRI (T2) ( update )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.