
Mirizzi syndrome
Updates to Article Attributes
Mirizzi syndrome refers to an uncommon phenomenon that results in extrinsic compression of an extrahepatic biliary duct from one or more calculi within the cystic duct or gallbladder. It is a functional hepatic syndrome but can often present with biliary duct dilatation and can mimic other hepatobiliary pathologies such as cholangiocarcinoma 2.
Epidemiology
The syndrome occurs in approximately 1 in every 1000 patients with gallstones 8.
Clinical presentation
Patients may present with recurrent episodes of jaundice and cholangitis. It can be associated with acute cholecystitis.
Pathology
Risk factors
A low insertion of the cystic duct into the common bile duct as well as a tortuous cystic duct are thought to be risk factors.
Classification
Management decisions depend on the type of Mirizzi syndrome 6,9 . A few classification systems have been proposed:
Csendes classification
-
type I: extrinsic compression of the common hepatic duct (CHD)
type Ia: by impacted gallstone in the gallbladder neck or cystic duct
type Ib: if cystic duct is absent 7
type II: erosion of CHD wall and formation of cholecystocholedochal fistula (up to one-third CHD wall circumference is involved)
type III: up to two-thirds of CHD wall circumference is involved in a cholecystocholedochal fistula
type IV: entire CHD wall is involved in a cholecystocholedochal fistula
type V: any of the above with cholecysto-enteric fistula 6
Beltrán classification
type I: external compression of the bile duct
-
type II: cholecystobiliary fistula
type IIa: less than 50% the diameter of the bile duct
type IIb: greater than 50% the diameter of the bile duct
-
type III: cholecystobiliary fistula and cholecystoenteric fistula
type IIIa: without gallstone ileus
type IIIb: with gallstone ileus
Radiographic features
Fluoroscopy
On ERCP, the stricture is smooth and often concave to the right ref.
CT
The gallbladder wall may be diffusely thickened and may enhance with contrast ref.
MRI
MRCP classically shows a large impacted gallstone in the gallbladder neck or cystic duct, or signs of inflamed gallbladder causing proximal dilatation of the extra and intrahepatic biliary tree, with distal gradual tapering of the extrahepatic biliary duct calibre to the site of obstruction ref.
Complications
FistulaeProlonged biliary obstruction and inflammation can develop between the gallbladder and the common duct, and the stone may pass into the common duct. lead to:
If the stone pass into the small bowl, it can develop intogallstone ileus 6.: if the stone passes into the small bowel through cholecysto-enteric fistulasecondary biliary cirrhosis 10
delayed onset biliary stricture10
History and etymology
This syndrome was first described by Pablo Luis Mirizzi (1893-1964), an Argentinian surgeon in a paper from 1940, although 1948 is often quoted, as in this year he published a paper in which it became widely-known 4,6. Mirizzi performed the first operative cholangiogram in 1931. He was named a Master Surgeon (Cirujano Maestro) in 1956 by the Argentinian Surgeons Society (Sociedad Argentina de Cirugía) 6.
-</ul><h4>Radiographic features</h4><h5>Fluoroscopy</h5><p>On ERCP, the stricture is smooth and often concave to the right <sup>ref</sup>.</p><h5>CT</h5><p>The gallbladder wall may be diffusely thickened and may enhance with contrast <sup>ref</sup>.</p><h5>MRI</h5><p><a href="/articles/magnetic-resonance-cholangiopancreatography-mrcp-2">MRCP</a> classically shows a large impacted gallstone in the gallbladder neck or cystic duct, or signs of inflamed gallbladder causing proximal dilatation of the extra and intrahepatic biliary tree, with distal gradual tapering of the extrahepatic biliary duct calibre to the site of obstruction <sup>ref</sup>. </p><h4>Complications</h4><p>Fistulae can develop between the gallbladder and the common duct, and the stone may pass into the common duct. </p><p>If the stone pass into the small bowl, it can develop into <a href="/articles/gallstone-ileus" title="Gallstone ileus">gallstone ileus</a> <sup>6</sup>.</p><h4>History and etymology</h4><p>This syndrome was first described by <strong>Pablo Luis Mirizzi</strong> (1893-1964), an Argentinian surgeon in a paper from 1940, although 1948 is often quoted, as in this year he published a paper in which it became widely-known <sup>4,6</sup>. Mirizzi performed the first operative cholangiogram in 1931. He was named a Master Surgeon (Cirujano Maestro) in 1956 by the Argentinian Surgeons Society (Sociedad Argentina de Cirugía) <sup>6</sup>.</p>- +</ul><h4>Radiographic features</h4><h5>Fluoroscopy</h5><p>On <a href="/articles/endoscopic-retrograde-cholangiopancreatography" title="ERCP">ERCP</a>, the stricture is smooth and often concave to the right <sup>ref</sup>.</p><h5>CT</h5><p>The gallbladder wall may be diffusely thickened and may enhance with contrast <sup>ref</sup>.</p><h5>MRI</h5><p><a href="/articles/magnetic-resonance-cholangiopancreatography-mrcp-2">MRCP</a> classically shows a large impacted gallstone in the gallbladder neck or cystic duct, or signs of inflamed gallbladder causing proximal dilatation of the extra and intrahepatic biliary tree, with distal gradual tapering of the extrahepatic biliary duct calibre to the site of obstruction <sup>ref</sup>. </p><h4>Complications</h4><p>Prolonged biliary obstruction and inflammation can lead to:</p><ul>
- +<li><p><a href="/articles/cholecystobiliary" title="cholecystobiliary fistula">cholecystobiliarry fistula</a>: leads to <a href="/articles/choledocholithiasis" title="Choledocholithiasis">choledocholithiasis</a> </p></li>
- +<li><p><a href="/articles/cholecystocutaneous-fistula" title="Cholecystocutaneous fistula">cholecystocutaneous fistula</a></p></li>
- +<li><p><a href="/articles/gallstone-ileus" title="Gallstone ileus">gallstone ileus</a> <sup>6</sup>: if the stone passes into the small bowel through <a href="/articles/cholecystoduodenal-fistula" title="Cholecystoduodenal fistula">cholecysto-enteric fistula</a></p></li>
- +<li><p>secondary biliary cirrhosis <sup>10</sup></p></li>
- +<li><p>delayed onset <a href="/articles/bile-duct-stricture" title="Biliary strictures">biliary stricture</a> <sup>10</sup></p></li>
- +</ul><h4>History and etymology</h4><p>This syndrome was first described by <strong>Pablo Luis Mirizzi</strong> (1893-1964), an Argentinian surgeon in a paper from 1940, although 1948 is often quoted, as in this year he published a paper in which it became widely-known <sup>4,6</sup>. Mirizzi performed the first operative cholangiogram in 1931. He was named a Master Surgeon (Cirujano Maestro) in 1956 by the Argentinian Surgeons Society (Sociedad Argentina de Cirugía) <sup>6</sup>.</p>
References changed:
- 10. Mark W. Jones & Troy Ferguson. Mirizzi Syndrome. StatPearls Publishing. 2022. <a href="https://www.ncbi.nlm.nih.gov/books/NBK482491/">https://www.ncbi.nlm.nih.gov/books/NBK482491/</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/29494098">Pubmed</a>
Image ( destroy )
Image 4 MRI (T2 fat sat) ( create )

Image 8 MRI (T2) ( create )

Image 9 MRI (FIESTA) ( create )
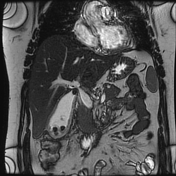
Image 10 MRI (T2) ( create )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.