
Ovarian fibrothecoma
Updates to Article Attributes
Ovarian fibrothecomas comprise tumours in the spectrum of ovarian sex cord / stromal tumours where there are components of both an ovarian fibroma and an ovarian thecoma.
Epidemiology
Most occur in adult women, with ~66% in postmenopausal women. Although they account for ~1% of all ovarian tumours 5, they are the most common benign solid ovarian tumour. It represents <2% of paediatric ovarian tumours.
Clinical presentation
The thecoma component of a fibrothecoma can secrete oestrogen, and the patient may present with abnormal vaginal bleeding and endometrial hyperplasia.
Pathology
These tumours have a variable amount of both fibrous tissue (see ovarian fibroma) and thecal cells (see ovarian thecoma).
Radiographic features
Ultrasound
They may be seen as a homogeneous hypoechoic mass with posterior acoustic shadowing, although in most cases the sonographic appearance is nonspecific.
CT
The vast majority (~80%) of ovarian fibrothecomas appear as solid masses with a delayed accumulation of contrast medium. On dynamic CT, there is an absence of arterial vessels and absence or slight early uptake of contrast enhancement 3. Calcification may be present and, as these tumours enlarge, myxoid or cystic degeneration may occur, resulting in a heterogeneous pattern 4.
MRI
Reported signal characteristics include 1:
- T1: typically shows homogeneous low signal intensity
-
T2
- lesions show predominantly homogeneous low signal intensity (from fibrous components)
- scattered high signal areas may be present, representing areas of cystic degeneration +/- oedema
Treatment and prognosis
Most cases are benign and surgical resection is curative.
Fibrothecomas are at risk for adnexal torsion, particularly with large tumours 4.As with pure ovarian fibromas, Meigs syndrome may complicate ~1% of cases
Differential diagnosis
-<li>scattered high signal areas may be present representing areas of cystic degeneration +/- oedema</li>- +<li>scattered high signal areas may be present, representing areas of cystic degeneration +/- oedema</li>
Image 1 MRI (T2) ( update )
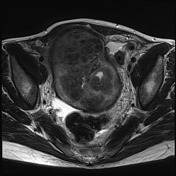
Image 3 MRI (T2) ( create )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.