
Transverse colon
Updates to Article Attributes
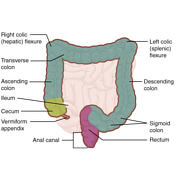
The transverse colon is the longest and most mobile part part of the large intestine. It measuremeasures up to 45cm45 cm in length.
Gross pathology and relationsanatomy
The transverse colon is the continuation of the ascending colon from the right colic flexure. It passes from the right to left hypochondrium in a downarddownward convex path crossing both the epigastric and umbilical zones. In the left hypochondrium hypochondrium, it curves sharply on itself beneath the lower end of the spleen, forming the left colic flexure.
It is almost completely invested by peritoneum, and is connected to the inferior border of the pancreas by a large and wide duplicature of that membrane, the transverse mesocolon. The gastrocolic ligament also attaches the transverse colon to the stomach.
Relations
- superiorly (right to left)
-: liver, gallbladder, greater curvature of the stomach, spleen - inferiorly: small bowel
- anteriorly
-: greater omentum and anterior abdominal wall - posteriorly (right to left)
- 2nd: 2nd part duodenum, head of pancreas, small bowel
Blood supply
- arterial
- middle colic artery (branch of superior mesenteric artery) supplies proximal 2/3
- ascending branch of left colic artery (branch of IMA) - supplies distal 1/3
- venous
-- via similarly named veins to splenic vein to the portal venous system
Nerve supply
- sympathetic
- superior mesenteric plexus
- inferior mesenteric plexus
- parasympathetic - derived from pelvic splanchnic nerves (S2-S4)
Lymphatic supplydrainage
Lymphatics accompany vessels and rain to paracolic nodes to the superior mesenteric group (proximal two-thirds) and inferior mesenteric group (distal two-thirds).
Radiological appearanceRadiographic features
Fluoroscopy
Double contrast barium enemas provided good anatomical detail from the rectum to the caecum. The patient may need to be rolled into various positions to get the barium to coat the lumen of the colon.
-<p>The <strong>transverse colon</strong> is the longest and most mobile part of the <a href="/articles/large-intestine-1">large intestine</a>. It measure up to 45cm in length. </p><h4>Gross pathology and relations</h4><p>The transverse colon is the continuation of the <a href="/articles/ascending-colon">ascending colon</a> from the <a href="/articles/right-colic-flexure">right colic flexure</a>. It passes from the right to left hypochondrium in a downard convex path crossing both the epigastric and umbilical zones. In the left hypochondrium, it curves sharply on itself beneath the lower end of the spleen, forming the <a href="/articles/left-colic-flexure">left colic flexure</a>. </p><p>It is almost completely invested by <a href="/articles/peritoneum">peritoneum</a>, and is connected to the inferior border of the <a href="/articles/pancreas">pancreas</a> by a large and wide duplicature of that membrane, the <a href="/articles/transverse-mesocolon">transverse mesocolon</a>. The <a href="/articles/gastrocolic-ligament">gastrocolic ligament</a> also attaches the transverse colon to the stomach. </p><h5>Relations</h5><ul>-<li>superiorly (right to left) - <a href="/articles/couinaud-classification">liver</a>, <a href="/articles/gallbladder">gallbladder</a>, greater curvature of the <a href="/articles/stomach">stomach</a>, <a href="/articles/spleen-1">spleen</a>- +<p>The <strong>transverse colon</strong> is the longest and most mobile part of the <a href="/articles/large-intestine-1">large intestine</a>. It measures up to 45 cm in length. </p><h4>Gross anatomy</h4><p>The transverse colon is the continuation of the <a href="/articles/ascending-colon">ascending colon</a> from the <a href="/articles/right-colic-flexure">right colic flexure</a>. It passes from the right to left hypochondrium in a downward convex path crossing both the epigastric and umbilical zones. In the left hypochondrium, it curves sharply on itself beneath the lower end of the spleen, forming the <a href="/articles/left-colic-flexure">left colic flexure</a>. </p><p>It is almost completely invested by <a href="/articles/peritoneum">peritoneum</a>, and is connected to the inferior border of the <a href="/articles/pancreas">pancreas</a> by a large and wide duplicature of that membrane, the <a href="/articles/transverse-mesocolon">transverse mesocolon</a>. The <a href="/articles/gastrocolic-ligament">gastrocolic ligament</a> also attaches the transverse colon to the stomach. </p><h5>Relations</h5><ul>
- +<li>superiorly (right to left): <a href="/articles/couinaud-classification">liver</a>, <a href="/articles/gallbladder">gallbladder</a>, greater curvature of the <a href="/articles/stomach">stomach</a>, <a href="/articles/spleen-1">spleen</a>
-<li>inferiorly - <a href="/articles/small_bowel(textbook)">small bowel</a>- +<li>inferiorly: <a href="/articles/small-bowel">small bowel</a>
-<li>anteriorly - <a href="/articles/greater-omentum">greater omentum</a> and <a href="/articles/anterior-abdominal-wall">anterior abdominal wall</a>- +<li>anteriorly: <a href="/articles/greater-omentum">greater omentum</a> and <a href="/articles/anterior-abdominal-wall">anterior abdominal wall</a>
-<li>posteriorly (right to left) - 2nd part <a href="/articles/duodenum">duodenum</a>, head of <a href="/articles/pancreas">pancreas</a>, <a href="/articles/small_bowel(textbook)">small bowel</a>- +<li>posteriorly (right to left): 2nd part <a href="/articles/duodenum">duodenum</a>, head of <a href="/articles/pancreas">pancreas</a>, <a href="/articles/small-bowel">small bowel</a>
-<li>venous - via similarly named veins to <a href="/articles/splenic-vein">splenic vein</a> to the <a href="/articles/portal-venous-system">portal venous system</a>- +<li>venous<ul><li>via similarly named veins to <a href="/articles/splenic-vein">splenic vein</a> to the <a href="/articles/portal-venous-system">portal venous system</a>
- +</li></ul>
-</ul><h4>Lymphatic supply</h4><p>Lymphatics accompany vessels and rain to paracolic nodes to the superior mesenteric group (proximal two-thirds) and inferior mesenteric group (distal two-thirds).</p><h4>Radiological appearance</h4><h5>Fluoroscopy</h5><p>Double contrast barium enemas provided good anatomical detail from the rectum to the caecum. The patient may need to be rolled into various positions to get the barium to coat the lumen of the colon. </p>- +</ul><h4>Lymphatic drainage</h4><p>Lymphatics accompany vessels and rain to paracolic nodes to the superior mesenteric group (proximal two-thirds) and inferior mesenteric group (distal two-thirds).</p><h4>Radiographic features</h4><h5>Fluoroscopy</h5><p>Double contrast barium enemas provided good anatomical detail from the rectum to the caecum. The patient may need to be rolled into various positions to get the barium to coat the lumen of the colon. </p>
Image ( destroy )
Image 1 Diagram ( create )





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.