
Truncus arteriosus
Updates to Article Attributes
Truncus arteriosus is a cyanotic congenital heart anomaly in which a single trunk supplies both the pulmonary and systemic circulation, instead of a separate aorta and a pulmonary trunk. It is usually classified as a conotruncal anomaly.
It accounts for up to 2% of congenital cardiac anomalies and is almost always associated with a ventricular septal defect (VSD) to allow circulatory flow circuit completion 1.
Epidemiology
The estimated incidence is 1 in 10,000 births.
Clinical presentation
Patients may present with signs/symptoms of cyanosis or congestive heart failure.
Pathology
There is a lack of normal separation of the embryological truncus arteriosus into a separate aorta and pulmonary trunk. This results in a single arterial vessel that originates from the heart that supplies the systemic, pulmonary and coronary circulations. It may also result in a common truncal valve which can contain 2-4 cusps.
Classifications
Collett and Edwards system
- type I: (most common) both aorta and main pulmonary artery arise from a common trunk
- type II: pulmonary arteries arise separately from the posterior aspect of trunk, close to each other just above the truncal valve (negligible main pulmonary artery segment)
- type III: (least common) pulmonary arteries arise independently from either side of trunk
- type IV: neither pulmonary arterial branch arising from the common trunk (pseudotruncus), currently considered a form of pulmonary atresia with a VSD
Van Praagh system
- type A1: identical to the type I of Collett and Edwards
- type A2: separate origins of the branch pulmonary arteries from the common trunk
- type A3: origin of one branch pulmonary artery (usually the right) from the common trunk, with other lung supplied either by collaterals or a pulmonary artery arising from the aortic arch
- type A4: presence of an associated interrupted aortic arch
Associations
- right sided aortic arch
- interrupted aortic arch 8
- persistence of primitive aortic arches
- DiGeorge syndrome
- CHARGE syndrome 11
Radiographic features
Chest radiograph
Often shows moderate cardiomegaly with pulmonary plethora (mainly as a result of collateral formation) and widened mediastinum.
However, the main pulmonary artery (arising from common trunk) may be small/unusual in position which may result in narrow mediastinum. This along with moderate cardiomegaly and pulmonary plethora gives an appearance that is similar to D-loop transposition of great arteries 9.
Right-sided aortic arch may be seen in ~40% (range 35-50%) of cases 2,10.
Echocardiography/prenatal ultrasound
Allows direct visualisation of a single trunk. Outflow tract views are the most useful. Colour Doppler may additionally show flow across both ways through an associated VSD.
CT/CTA
Allows direct visualisation of anomalous anatomy.
MRI
Allows direct visualisation of anomalous anatomy. SSFP cine sequences can offer additional functional assessment.
Treament and pognosis
Due to parallel fetal circulation, truncus arteriosus does not cause any haemodynamic problem in utero. However it is a major problem postnatally and, if left untreated, approximately 80% of infants die within the first year.
Differential diagnosis
-<a title="CHARGE syndrome" href="/articles/charge-syndrome">CHARGE syndrome</a> <sup>11</sup>- +<a href="/articles/charge-syndrome">CHARGE syndrome</a> <sup>11</sup>
Image 7 CT (C+ arterial phase) ( update )

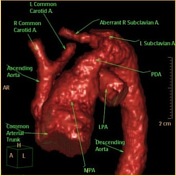
Image 8 CT (Annotated images) ( update )





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.