
X-linked adrenoleukodystrophy
Updates to Article Attributes
Adrenoleukodystrophy (ALD) is one of the x-linked congenital dysmyelinating diseases.
Epidemiology
The estimated incidence is at around 1:20,000-50,000. Due to its X-linked inheritance it classically affects young males.
Pathology
The conditions results from an accumulation of very long chain fatty acids (VLCFAs) from a genetic deficiency in peroxisomal oxidation of fatty acids. This is thought to result from a mutation in a ALDP gene located on Xq28 5. The cerebral white matter is typically split into three different zones:
- central (inner) zone: irreversible gliosis and scarring
- intermediate zone: active inflammation and breakdown of the blood-brain barrier
- peripheral (outer) zone: leading edge of active demyelination
Phenotypes
There are five main phenotypes 3:
- childhood cerebral
- adolescent cerebral
- adult cerebral
- AMN
- limited to Addison's disease
Some individuals can be asymptomatic.
Radiographic features
MRI
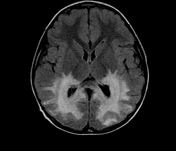
A majority of cases tend to show symmetrical cerebral white matter signal change involving the posterior periventricular white matter (i.e. posterior cerebral, around splenium and peritrigonal white matter). Signal changes can vary according to the zonal distribution within the affected white matter. There is relative sparing of subcortical U-fiber involvement.
-
T1
- central zone: hypo-intense
- intermediate zone
- peripheral zone
-
T1 C+ (Gd)
- enhancement seen in around 50% of cases according to one study and is thought to be associated with disease progression 6
- with contrast infusion, serpiginous, garland-shaped enhancement may be visible in the anterior most periphery of the lesions 7
-
T2
- central zone: markedly hyperintense
- intermediate zone: isointense to hypointense
- peripheral zone: moderately hypointense
MR spectroscopy
Spectroscopy may show evidence of neuronal loss manifested by a decrease in the NAA peak and an elevation in the lactate peak.
Treatment and prognosis
Bone marrow transplantation is thought to be favourable in the early stages of disease. Restriction of VLCFAs has also been trialled.
Differential diagnosis
Differential consideration for the classic pattern include:
- acetyl CoA oxidase deficiency (pseudo adrenoleukodystrophy): has a different clinical presentation
EtymologyHistory and etymology
It is thought to have originally been described by Siemerling and Creutzfeld in 1923 1.
-<a href="/articles/acetyl-coa-oxidase-deficiency">acetyl CoA oxidase deficiency</a> (<a href="/articles/pseudo-adrenoleukodystrophy">pseudo a</a><a href="/articles/pseudo-adrenoleukodystrophy">drenoleukodystrophy</a>): has a different clinical presentation</li></ul><h4>Etymology</h4><p>It is thought to have originally been described by <strong>Siemerling</strong> and <strong>Creutzfeld</strong> in 1923 <sup>1</sup>.</p>- +<a href="/articles/acetyl-coa-oxidase-deficiency">acetyl CoA oxidase deficiency</a> (<a href="/articles/pseudo-adrenoleukodystrophy">pseudo a</a><a href="/articles/pseudo-adrenoleukodystrophy">drenoleukodystrophy</a>): has a different clinical presentation</li></ul><h4>History and etymology</h4><p>It is thought to have originally been described by <strong>Siemerling</strong> and <strong>Creutzfeld</strong> in 1923 <sup>1</sup>.</p>
Image 10 MRI (FLAIR) ( create )





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.