
Papillary thyroid cancer
Updates to Article Attributes
Papillary thyroid carcinoma (PTC) is the most common malignancy of the thyroid gland, and frequently has nodal metastases at presentation.
Epidemiology
Papillary thyroid cancer (as is the case with follicular thyroid cancer) typically occurs in the middle-aged, with a peak incidence in the 3rd and 4th decades. It is more common in women with a F:M ratio of 1:1.6 - 3:1 2.
It accounts for the majority (approximately 70%) of all thyroid neoplasms and 85% of all thyroid cancers 2,4. There are 45,000 cases in the United States every year and this type of carcinoma has the fastest increasing incidence of any malignancy in the thyroid. Those at risk include a family history and previous head/ neck radiation.
Clinical presentation
Presentation is usually with a solitary palpable thyroid mass.
Papillary carcinoma has a tendency to metastasise early to local lymph nodes, with 50% (39-90% 2) of patients having nodal involvement at presentation 1 (cf. 10% for follicular thyroid cancer). These metastases are usually to the ipsilateral jugular chain (87.8%) and are usually confined to the mid and lower lymph node levels, level III and IV (73.2%) 1.
In ~20% of patients, lymph node metastases are the first presentation. In 50% of children and 20% of adults a cervical lymph node is palpable at the time of diagnosis 4.
Distal haematogeneous dissemination is less common than with follicular cancer, with a prevalence of only in 5-10% of patients at presentation.
Pathology
Histologically papillary carcinoma demonstrates 'delicate stalks of epithelial cells' 3 which account for its name. Cells have characteristic Orphan Annie eye nuclear inclusions, and psammoma bodies are common.
Lymphatic spread is more common than haematogeneous spread (c.f. follicular thyroid carcinoma) and multifocality is common.
Associations
Radiographic features
Imaging of the neck of a patient with papillary thyroid carcinoma involves both examination of the thyroid as well as careful assessment of the regional lymph nodes for the presence of metastases.
Ultrasound
Papillary carcinoma within the thyroid usually appears as a solitary mass usually with an irregular outline, located in the subcapsular region and demonstrating vascularity 6. Small punctate regions of echogenicity representing microcalcifications (psammoma bodies) may be present 5.
Lymph node metastases have a tendency to completely cavitate (40%), and although usually multiple, in a minority of cases (6%) a single completely cystic node may be present 1. They tend to have septations, mural nodules and relatively thick walls 1.
Very few radiologists would aspirate a lesion under 10 mm in diameter for 3 reasons: small solid lesions under 10 mm are very common in the general population (and often often multiple. Depending on which reference you use, up to 50% of the general population will have thyroid nodules of some description on high resolution thyroid ultrasound 9) , the possibility of sampling error and patient distress.
A lesion that enlarges with follow up is a relatively strong indication for FNA of the lesion. In patients with pathological cervical nodes on ultrasound, any thyroid lesion should likely be aspirated.
In every day ultrasound practice, PTC most commonly has poorly defined margins and/or calcifications (which may be macrocalcifications). There is a poor correlation between blood flow and malignancy in practice. Aspiration of simple cysts of the thyroid lesions does not yield malignant cells and cysts can safely be followed up in the context of excluding malignancy.
CT
CT is best at staging lymph node involvement (see thyroid cancer staging). Involved lymph nodes tend to have 1:
- cystic components: ~35%
- thick nodular walls: ~40%
- septa: ~60%
- purely cystic nodes are uncommon and more frequent in young patients
- calcification may be seen occasionally
- the so-called lateral aberrant thyroid is actually a lymph node metastasis from papillary thyroid carcinoma
MRI
MRI, although probably more sensitive that CT, is nonetheless still far from perfect with a sensitivity of only 67% 2. This is largely a result of the fact that as many as half involved nodes found histologically following surgery, being less than 3 mm in diameter 2.
As discussed above, nodes have a tendency to become cystic. The cystic component will have near-fluid attenuation. The solid metastatic component will appear 2:
General signal characteristics include:
-
T1
- hypointense cf. muscle
- enhancement best seen with fat suppression
-
T2: variable 2
- hypointense: 34%
- isointense: 45%
- hyperintense: 21%
Nuclear imaging
Papillary thyroid cancer usually concentrates radioiodine, but not pertechnetate.
-
FDG-PET
- FDG-avid
- incidental FDG-avid thyroid nodules have ~40% risk of being a primary thyroid malignancy 9.
Treatment and prognosis
Treatment involves both surgical resection and administration of radioactive iodine for lymph node metastases.
Overall papillary carcinoma carries a relatively good prognosis with a 20 year survival rate of approximately 90%. The 5 year survival is in the range of 95%. If the tumour is confined to the gland then mortality is less than 2.5%, with a sharp increase in mortality in patients with extension beyond the gland, to 38% 2.
Differential diagnosis
Other thyroid neoplasms should be considered in the absence of cavitary cervical lymph nodes.
The differential of a cystic neck mass(es) includes:
- thyroglossal duct cyst (only if single)
- branchial cleft cyst (only if single)
- cystic metastasis
- abscess including tuberculous lymphadenitis
- multiple neurofibromas
-<strong>T2:</strong> variable <sup>2</sup><ul>- +<strong>T2</strong>: variable <sup>2</sup><ul>
References changed:
- 9. Chung A, Tran T, Brumund K, Weisman R, Bouvet M. Metastases to the Thyroid: A Review of the Literature from the Last Decade. Thyroid. 2012;22(3):258-68. <a href="https://doi.org/10.1089/thy.2010.0154">doi:10.1089/thy.2010.0154</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/22313412">Pubmed</a>
- 9. 3. Chung AY, Tran TB, Brumund KT et-al. Metastases to the thyroid: a review of the literature from the last decade. Thyroid. 2012;22 (3): 258-68. <a href="http://dx.doi.org/10.1089/thy.2010.0154">doi:10.1089/thy.2010.0154</a> - <a href="http://www.ncbi.nlm.nih.gov/pubmed/22313412">Pubmed citation</a><span class="auto"></span>
Image ( update )
Image 1 Photo (Cut gross specimen) ( update )

Image 2 Pathology (H&E) ( update )

Image 3 CT (liver window) ( update )

Image 4 CT (C+ arterial phase) ( update )

Image 5 CT (C+ arterial phase) ( update )

Image 6 MRI (STIR) ( update )
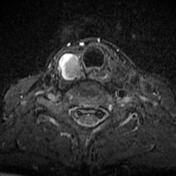
Image 7 Annotated image ( update )

Image 8 MRI (T1) ( update )

Image 9 Ultrasound (Longitudinal) ( update )

Image 10 CT (C+ portal venous phase) ( update )
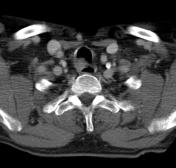
Image 11 Ultrasound ( update )

Image 13 Ultrasound (Long/Tra) ( update )

Image 14 CT (lung window) ( update )

Image 15 Ultrasound (Trans and long) ( update )

Image 16 CT (lung window) ( update )

Image 17 Ultrasound (Transverse) ( update )
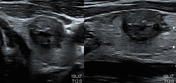
Image 24 Ultrasound (Trans and long) ( update )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.